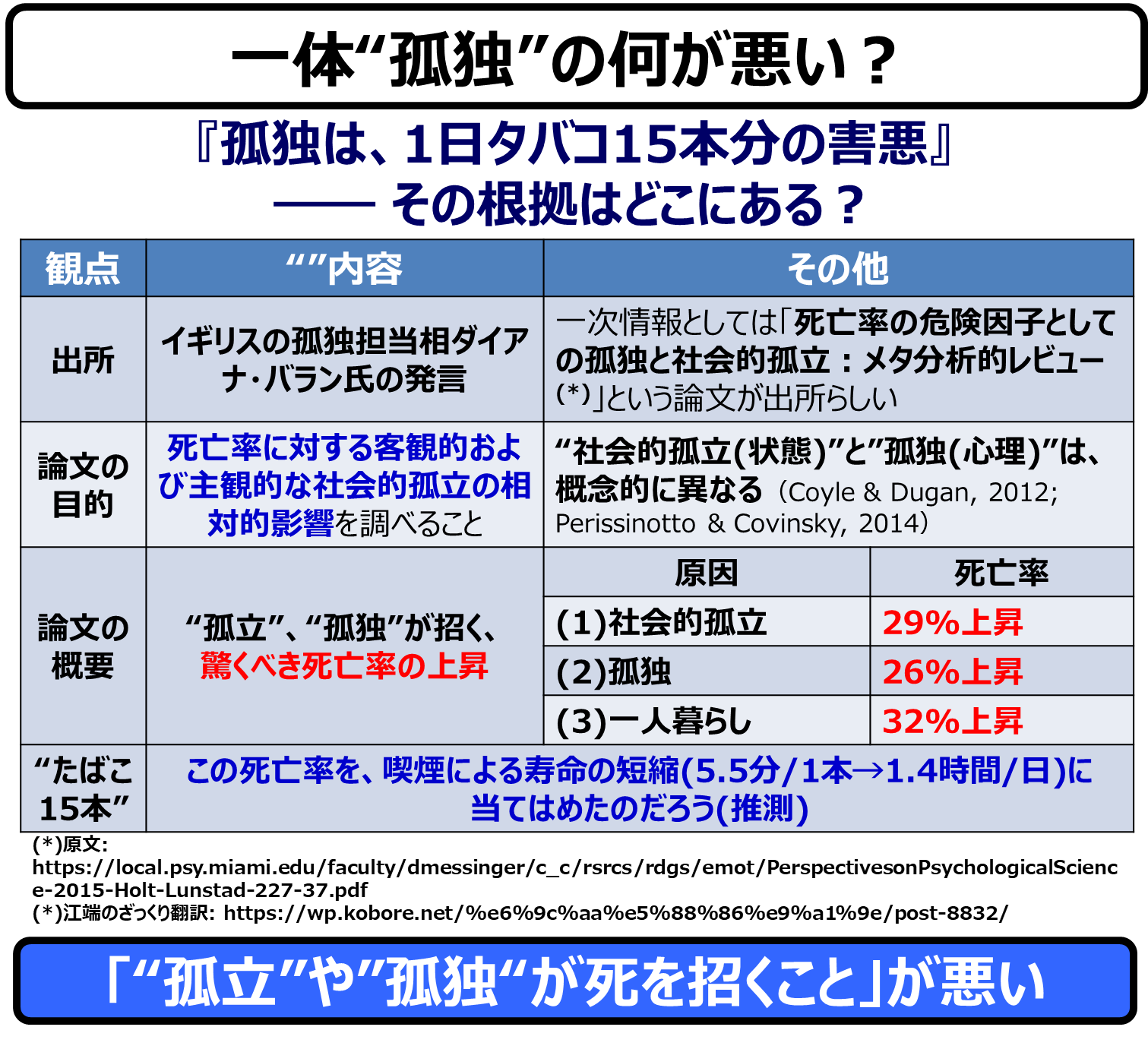
Actual and perceived social isolation are both associated with increased risk for early mortality. In this meta-analytic review, our objective is to establish the overall and relative magnitude of social isolation and loneliness and to examine possible moderators. We conducted a literature search of studies (January 1980 to February 2014) using MEDLINE, CINAHL, PsycINFO, Social Work Abstracts, and Google Scholar. The included studies provided quantitative data on mortality as affected by loneliness, social isolation, or living alone. Across studies in which several possible confounds were statistically controlled for, the weighted average effect sizes were as follows: social isolation odds ratio (OR) = 1.29, loneliness OR = 1.26, and living alone OR = 1.32, corresponding to an average of 29%, 26%, and 32% increased likelihood of mortality, respectively. We found no differences between measures of objective and subjective social isolation. Results remain consistent across gender, length of follow-up, and world region, but initial health status has an influence on the findings. Results also differ across participant age, with social deficits being more predictive of death in samples with an average age younger than 65 years. Overall, the influence of both objective and subjective social isolation on risk for mortality is comparable with well-established risk factors for mortality.
------
実際の社会的孤立と認識された社会的孤立は、ともに早期死亡のリスク上昇と関連している。このメタ分析レビューでは、社会的孤立と孤独の全体的および相対的な大きさを確定し、可能なモデレーターを検討することを目的としている。MEDLINE、CINAHL、PsycINFO、Social Work Abstracts、Google Scholarを用いて、研究の文献検索(1980年1月~2014年2月)を行った。対象とした研究は、孤独感、社会的孤立、一人暮らしが影響する死亡率に関する定量的データを提供していた。いくつかの可能性のある交絡因子が統計的にコントロールされた研究全体で、加重平均効果量は以下の通りであった:社会的孤立のオッズ比(OR)=1.29、孤独のOR=1.26、一人暮らしのOR=1.32、これはそれぞれ平均29%、26%、32%の死亡率の上昇に対応している。客観的な社会的孤立と主観的な社会的孤立の測定値に差は見られなかった。結果は、性別、追跡期間、地域によって一貫しているが、初期の健康状態が結果に影響を及ぼしている。結果は参加者の年齢によっても異なり、平均年齢が65歳未満のサンプルでは、社会的欠陥が死亡をより予測することがわかった。全体として、死亡リスクに対する客観的および主観的な社会的孤立の影響は、死亡に対する確立された危険因子と同等である。
------
Keywords
social isolation, loneliness, mortality
------
キーワード
社会的孤立、孤独、死亡率
------
Several lifestyle and environmental factors are risk factors for early mortality, including smoking, sedentary lifestyle, and air pollution. However, in the scientific literature, much less attention has been given to social factors demonstrated to have equivalent or greater influence on mortality risk (Holt-Lunstad, Smith, & Layton, 2010). Being socially connected is not only influential for psychological and emotional well-being but it also has a significant and positive influence on physical well-being (Uchino, 2006) and overall longevity (Holt-Lunstad et al., 2010; House, Landis, & Umberson, 1988; Shor, Roelfs, & Yogev, 2013). A lack of social connections has also been linked to detrimental health outcomes in previous research. Although the broader protective effect of social relationships is known, in this meta-analytic review, we aim to narrow researchers’ understanding of the evidence in support of increased risk associated with social deficits. Specifically, researchers have assumed that the overall effect of social connections reported previously inversely equates with risk associated with social deficits, but it is presently unclear whether the deleterious effects of social deficits outweigh the salubrious effects of social connections. Currently, no meta-analyses focused on social isolation and loneliness exist in which mortality is the outcome. With efforts underway to identify groups at risk and to intervene to reduce that risk, it is important to understand the relative influence of social isolation and loneliness.
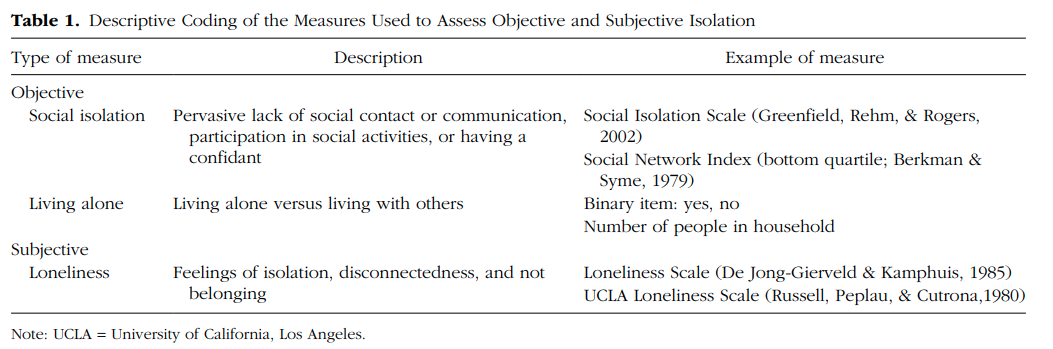
Living alone, having few social network ties, and having infrequent social contact are all markers of social isolation. The common thread across these is an objective quantitative approach to establish a dearth of social contact and network size. Whereas social isolation can be an objectively quantifiable variable, loneliness is a subjective emotional state. Loneliness is the perception of social isolation, or the subjective experience of being lonely, and thus involves necessarily subjective measurement. Loneliness has also been described as the dissatisfaction with the discrepancy between desired and actual social relationships (Peplau & Perlman, 1982). Is there a need to distinguish between social isolation and loneliness in assessing mortality risk? People lacking human contact often feel lonely (Yildirim & Kocabiyik, 2010); however, social isolation and loneliness are often not significantly correlated (Coyle & Dugan, 2012; Perissinotto & Covinsky, 2014), suggesting that these may be independent constructs and that one may occur without the other. For instance, some may be socially isolated but content with minimal social contact or actually prefer to be alone; others may have frequent social contact but still feel lonely. Because of the conceptual distinction between social isolation and loneliness, understanding their relative influence on mortality may provide insights into possible independent pathways by which each influences risk and, in turn, guides intervention efforts.
There are several processes by which actual and perceived social isolation may influence mortality risk (also see other reviews in this special section). Social connections, or the lack thereof, can influence health and risk of mortality via direct and indirect pathways (see Uchino, 2006). Both loneliness and social isolation are associated with poorer health behaviors including smoking, physical inactivity, and poorer sleep (Cacioppo et al., 2002; Hawkley, Thisted, & Cacioppo, 2009; Theeke, 2010). Each is also associated with health-relevant biological processes, including higher blood pressure, C-reactive protein, lipid profiles, and poorer immune functioning (Grant, Hamer, & Steptoe, 2009; Hawkley & Cacioppo, 2010; Pressman et al., 2005). Researchers that have included both social isolation and loneliness have linked these factors independently to poorer health behaviors and biological risk factors (Pressman et al., 2005; Shankar, McMunn, Banks, & Steptoe, 2011). However, few researchers have examined these concurrently, and little is known about their relative or synergistic influence. In this meta-analytic review, our primary aim was to focus on the relative effects of objective and subjective social isolation on mortality (the likelihood of death over a given time), to determine the magnitude and nature of the association with risk of mortality, and to identify potential moderating variables. We reviewed studies of mortality that included measures of loneliness, social isolation, or living alone. Because it is important to determine the effect of social isolation and loneliness independent of correlated lifestyle (e.g., smoking, physical activity) and psychological factors (e.g., depression, anxiety), we also examined inclusion of covariates.
------
実際の社会的孤立や社会的孤立の認知が死亡率に影響を与えるプロセスはいくつかある(本特集の他のレビューも参照のこと)。社会的なつながり、あるいはその欠如は直接的、間接的な経路で健康や死亡リスクに影響を与える可能性がある(Uchino, 2006参照)。孤独と社会的孤立はともに、喫煙、運動不足、睡眠不足など、より悪い健康行動と関連している (Cacioppo et al., 2002; Hawkley, Thisted, & Cacioppo, 2009; Theeke, 2010)。また、血圧の上昇、CRP、脂質プロファイル、免疫機能の低下など、健康に関連する生物学的過程とも関連している(Grant, Hamer, & Steptoe, 2009; Hawkley & Cacioppo, 2010; Pressman et al.) 社会的孤立と孤独の両方を含む研究者は、これらの要因をより悪い健康行動や生物学的危険因子と独立して結びつけています(Pressman et al.、2005;Shankar、McMunn、Banks、& Steptoe、2011)。しかし、これらを同時に検討した研究者は少なく、これらの相対的あるいは相乗的な影響についてはほとんど知られていない。このメタ分析レビューでは、死亡率(一定期間内に死亡する可能性)に対する客観的・主観的社会的孤立の相対的影響に焦点を当て、死亡リスクとの関連の大きさと性質を明らかにし、潜在的な緩和変数を特定することを主目的とした。我々は、孤独感、社会的孤立、一人暮らしの尺度を含む死亡率に関する研究をレビューした。社会的孤立や孤独の影響を、相関するライフスタイル(例:喫煙、身体活動)や心理的要因(例:うつ病、不安)から独立して判断することが重要であるため、共変数を含むかどうかも検討した。
------
Method
方法
------
Identification of studies
研究の特定
------
We identified published and unpublished studies of the association between social relationships and mortality using two techniques. First, we searched for studies appearing from January 1980 to February 2014 using several electronic databases: MEDLINE, CINAHL, PsycINFO, Social Work Abstracts, and Google Scholar. To capture relevant articles, we used multiple search terms, including mortality, death, decease(d), died, dead, and remain(ed) alive, which were crossed with synonyms of the terms social isolation, loneliness, and living alone. To minimize inadvertent omissions, we searched each database twice, with searches ending on February 24, 2014. Second, we manually examined the reference sections of past reviews and of studies meeting the inclusion criteria to locate articles not identified in the database searches. A team of research assistants who were trained and supervised by the authors conducted the searches.
------
社会的関係と死亡率の関連について、2つの手法で公表済みおよび未公表の研究を同定した。まず、1980年1月から2014年2月までに出現した研究を、いくつかの電子データベースを用いて検索した。MEDLINE、CINAHL、PsycINFO、Social Work Abstracts、およびGoogle Scholarである。関連する論文を捉えるために、mortality, death, decease(d), died, dead, remain(ed) aliveなどの複数の検索語を用い、social isolation, loneliness, living aloneの同義語と掛け合わせた。不用意な脱落を最小限にするため、各データベースを2回検索し、検索は2014年2月24日に終了した。次に,データベース検索で特定されなかった論文を見つけるために,過去のレビューや包括基準を満たした研究の参考文献のセクションを手作業で調査した。検索は,著者らによって訓練・指導されたリサーチアシスタントのチームが行った。
------
Inclusion criteria
対象基準
------
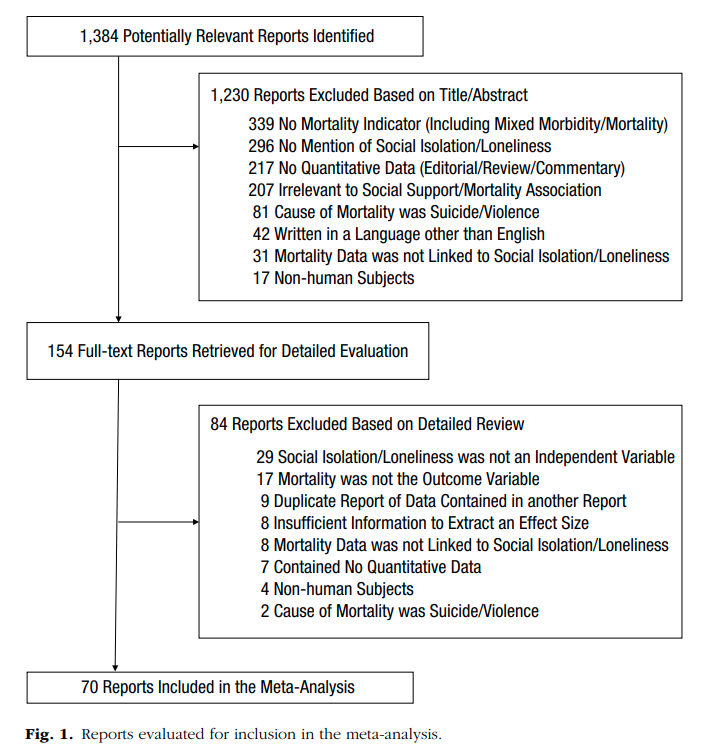
We included in the meta-analysis studies written in English that provided quantitative data regarding individuals’ mortality as a function of objective and subjective social isolation (operational definitions of social isolation, loneliness, and living alone are provided in Table 1). All studies needed to be prospective in design, meaning that the researchers measured one’s objective or subjective social isolation at the study initiation and then followed participants over time (typically several years) to determine who remained alive and who was dead at the follow-up. Thus, risk for mortality is an estimate of the extent to which social isolation, living alone, and loneliness significantly predict the likelihood of being dead at follow-up. We extracted data when authors used measures including the terms found in Table 1. In some cases, authors operationalized social isolation by contrasting the participants from the bottom quartile or quintile on a social network or integration measure (e.g., Social Network Index; Cohen, Doyle, Skoner, Rabin, & Gwaltney, 1997) but otherwise did not code data from measures of social networks/integration. Because we were interested in the impact of social deficits on disease, we excluded studies in which mortality was a result of suicide or accident. We also excluded studies in which the outcome could not be isolated to mortality (e.g., combined outcomes of morbidity and mortality). Although we excluded single-case designs and reports with exclusively aggregated data (e.g., census-level statistics), we included all other types of quantitative research designs that yielded a statistical estimate of the association between mortality and loneliness/isolation. Figure 1 shows the flow diagram containing the details of study inclusion (included in the Supplemental Material available online).
A team of research assistants and the authors performed the data searches and coding. To reduce the likelihood of human error in coding, a team of two raters coded each article twice. Two different raters performed the second coding of each article. Thus, two distinct coding teams (four raters) coded each article. Coders extracted several objectively verifiable characteristics of the studies: (a) the number of participants and their composition by age, gender, health status, and preexisting health conditions (if any), as well as the cause of mortality; (b) length of follow-up; (c) research design; (d) type of social isolation (actual/perceived) evaluated; (e) number and class of covariates included in the statistical model; and (f) exclusion of participants who were severely ill or who died shortly after study initiation. The latter two variables helped to address possible confounds (e.g., depression, health status, physical mobility, age) and reverse causality, whereby individuals with impaired health would be more likely to report increased social isolation or loneliness because of an inability to engage in social contact. For each study, we extracted the reported effect size, making sure that odds ratio (OR) values greater than one represented an increase in mortality as a function of social isolation, loneliness, or living alone?and a decrease in mortality when individuals were not isolated, lonely, or living alone. Effect sizes less than one indicated the opposite. To analyze the data, we temporarily transformed the reported effect sizes to the natural log of the OR and subsequently transformed them back to ORs for purposes of interpretation. When researchers reported multiple effect sizes within a study at the same point in time, we averaged the several values (weighted by standard error) to avoid violating the assumption of independent samples. We therefore used the shifting units of analysis approach (Cooper, 1998), which minimizes the threat of nonindependence in the data while allowing for more detailed follow-up analyses. In a few cases in which researchers reported multiple effect sizes across different levels of social isolation (high vs. medium, medium vs. low), we extracted only the value with the greatest contrast (high vs. low).
------
データ検索とコーディングは、リサーチアシスタントと著者のチームが行った。コーディングにおけるヒューマンエラーの可能性を減らすため、2 人の評価者チームが各論文を 2 回コーディン グした。各論文の 2 回目のコーディングは、異なる 2 名の評価者が行った。このように、2 つの異なるコーディングチーム(4 名の評価者)が各記事をコーディン グした。(a)参加者数、年齢、性別、健康状態、既往症(ある場合)、および死亡原因による構成、(b)追跡期間の長さ、(c)研究デザイン、(d)評価した社会的孤立(実際/知覚)の種類、(e)統計モデルに含めた共変量の数および種類、(f) 重病または研究開始後すぐに死亡した参加者の除外など、コーダーは研究の客観的検証を行ういくつかの特性を抜き出しました。後者の2つの変数は、起こりうる交絡因子(例:うつ病、健康状態、身体的移動性、年齢)および逆因果(健康障害のある人は、社会的接触ができないために社会的孤立や孤独の増加を報告する可能性が高い)に対処するのに役立つものである。各研究について、報告された効果量を抽出し、1より大きいオッズ比(OR)値が、社会的孤立、孤独、または一人暮らしの機能として死亡率の増加を表し、個人が孤立、孤独、または一人暮らしではない場合に死亡率が減少することを確認する。1未満の効果量は、その逆を表していた。データを分析するために、報告された効果量を一時的にORの自然対数に変換し、その後、解釈のためにORに変換しなおした。研究者が同じ時点の研究内で複数の効果量を報告した場合、独立標本の仮定に違反しないように、複数の値を平均化した(標準誤差で重み付け)。そのため、データにおける非独立性の脅威を最小限に抑えつつ、より詳細な追跡分析が可能なshifting units of analysis approach (Cooper, 1998)を使用した。研究者が異なる社会的孤立のレベル(高対中、中対低)で複数の効果量を報告しているいくつかのケースでは、最も対照的な値(高対低)のみを抽出した。
When a study contained multiple effect sizes across time, we extracted the data from the longest follow-up period. We extracted both unadjusted data and the data from the model involving the greatest number of statistical controls (although we also extracted the data from the model utilizing the fewest number of statistical controls for a subsequent comparison after recording the type and number of statistical controls used within both models). Overall, the interrater agreement for data abstraction was adequately high for categorical variables (with Cohen’s kappa averaging .73) and for continuous variables (with intraclass correlations for single measures averaging .95). We resolved discrepancies across coding teams through further scrutiny of the article until we obtained consensus.?
------
Results
成果
Description of the retrieved literature
検索した文献の説明
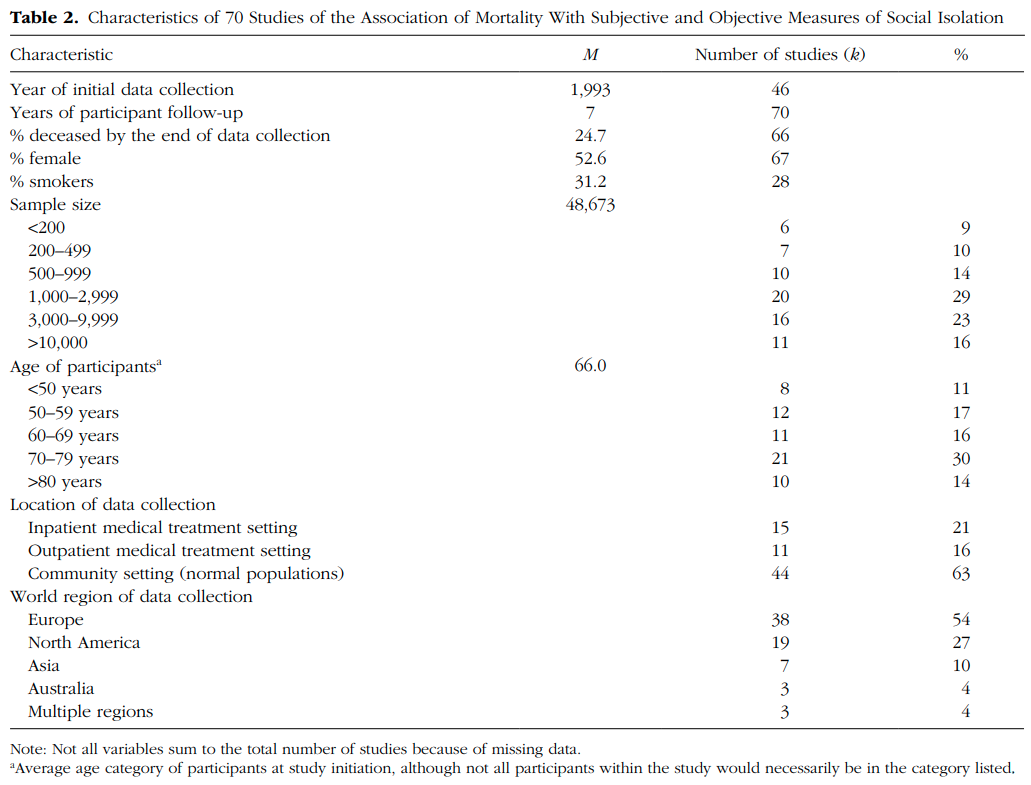
We located 79 articles reporting pertinent data, 9 of which were excluded because they contained the same data as another article, resulting in 70 independent studies that met the full inclusion criteria. The complete list of references and a table summarizing the characteristics of those studies (Table S1) are found in the Supplemental Material available online. Studies typically involved older adults, with a mean age of 66.0 years at initial data collection and with a mean length of follow-up being 7.1 years. Most studies (63%) involved normal community samples, but 37% of studies involved patients with a medical condition, such as heart disease. See Table 2 for further descriptive data. Three studies included data on both loneliness and one of the objective independent variables: two for loneliness and social isolation, and one for loneliness and living alone. Using a shifting units of analysis approach (Cooper, 1998), we included data from those distinct measures in the analyses specific to the type of measurement, but all other studies contributed a single data point to the analyses.
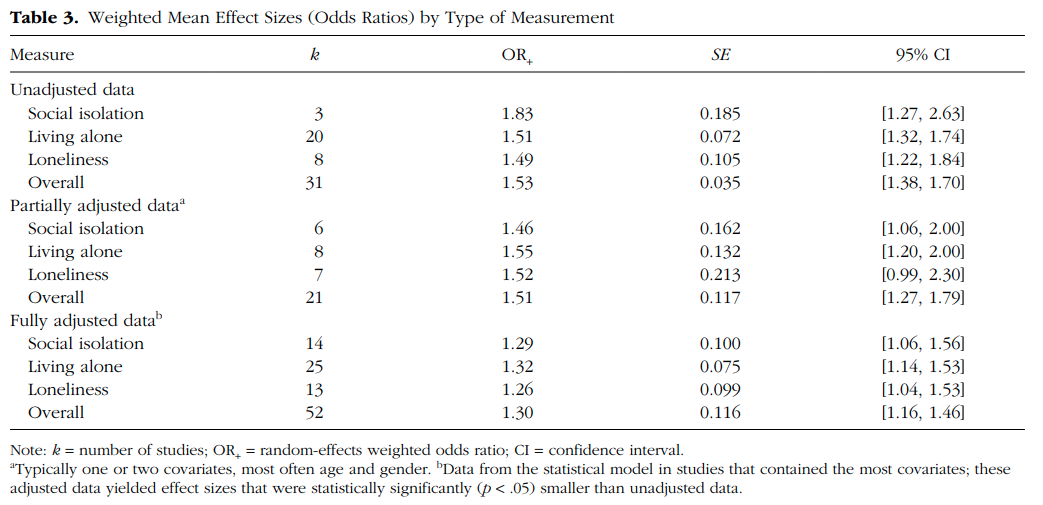
Effect sizes in the 70 studies had been calculated by researchers using a variety of methods, with some researchers reporting unadjusted values and with other researchers using a variety of covariates. ORs ranged from 0.64 to 3.85, with exceptionally high heterogeneity across studies (I 2 = 97.8%, 95% CI [97.6%, 98.1%]; Q = 3,328.9, p < .0001), suggesting excessive variability in findings across all types of data. We therefore divided the analyses according to the number of covariates used. In the unadjusted data group, the researchers controlled for no other variables in the analyses. In the partially adjusted data group, the researchers typically controlled for one or two variables, usually age and gender. The fully adjusted data are the model within studies with the largest number of covariates. Effect sizes from each category were evaluated separately, such that a single study could contribute effect sizes to more than one category (see Table 3).
------
70件の研究の効果量は、研究者によってさまざまな方法で計算されており、ある研究者は未調整値を報告し、他の研究者はさまざまな共変数を使用していた。ORは0.64から3.85の範囲で、研究間の異質性は例外的に高く(I 2 = 97.8%, 95% CI [97.6%, 98.1%]; Q = 3,328.9, p < .0001)、すべての種類のデータで所見が過度に変動していることが示唆された。そこで、使用した共変量の数によって解析を分けた。未調整データ群では、研究者は分析において他の変数を一切コントロールしなかった。部分調整データ群では、研究者は通常1つか2つの変数、通常は年齢と性別をコントロールした。完全調整データは、共変量が最も多い研究内のモデルである。各カテゴリーの効果量は別々に評価され、1つの研究が2つ以上のカテゴリーに効果量を寄与することもある(表3参照)。
------
------
Overall, each of the measures (social isolation, loneliness, and living alone) for each type of data (unadjusted, partially adjusted, or fully adjusted) had an OR between 1.26 and 1.83. The three measures did not differ in their ORs for any of the three types of data, meaning that there was no overall difference among the two objective and one subjective factors. (Random-effects weighted analyses of variance across the measures yielded all ps > .20.) However, the type of data did matter in the analysis. Unadjusted data yielded effect sizes of greater magnitude than fully adjusted data (see Table 3). The differences between unadjusted and fully adjusted data also reached statistical significance (p < .001) when comparing data within 27 studies in which researchers reported more than one statistical model (e.g., unadjusted compared with fully adjusted values) using multivariate meta-analytic methods after accounting for the .74 correlation of effect sizes within studies. Thus, unadjusted and fully adjusted data not only represented conceptually distinct classes of data but also yielded findings of different magnitude.
Given the substantial heterogeneity of the overall results (I 2 > 80%), we analyzed the extent to which the variability in effect sizes could be attributable to study or participant characteristics. These analyses involved only the fully adjusted data because multiple factors predictive of mortality had been controlled (thus minimizing possible confounding explanations). Study and participant characteristics included both categorical and continuous data, so we report those analyses separately.
We examined categorical variables using random-effects weighted analyses of variance, beginning with the type of covariates used in the fully adjusted models. Eight studies included multiple covariates that were directly relevant to social support, such as marital status, social networks, and loneliness. These eight studies had lower averaged effect sizes (OR = 1.17) than those of 33 studies in which no covariates directly relevant to social support were included in the statistical model (OR = 1.27). Otherwise, the averaged effect sizes remained of similar magnitude irrespective of the particular covariates that were or were not included in the models (p > .20), including covariates relevant to depression, socioeconomic status, health status, physical activity, smoking, gender, and age. Different combinations of covariates across studies yielded similar results. We found no substantive differences in effect sizes (p > .15) across the other categorical variables evaluated: world region, data collection setting, cause of mortality, research design, health status, and medical condition at intake. Finding no significant differences across participant health status when using the fully adjusted data was particularly notable because of a difference that we observed with the unadjusted data: Studies in which participants had a medical condition and were recruited from a medical setting had larger unadjusted average effect sizes (OR = 1.82) than studies with ostensibly healthy participants recruited from the general community (OR = 1.34, p = .003). Furthermore, with the unadjusted data, studies in which the researchers excluded participants with terminal conditions or participants who died shortly after baseline data collection (whose social isolation or social support may have been affected by their medical condition) had higher averaged effect sizes (OR = 1.95) than the studies in which the researchers did not report such exclusions (OR = 1.38, p < .05). Thus, accounting for participants’ initial health condition in the research design resulted in systematically different findings across studies. In most (81%) of the multivariate statistical models, researchers had controlled for participant health status variables, such that we found no differences across those conditions in the fully adjusted data. Studies in which the researchers controlled for health status variables yielded substantially different findings from those studies in which this was not done.
We examined study and participant characteristics involving continuous data in relation to the observed effect sizes using random-effects weighted regression coefficients (meta-regression). We observed no coefficients greater than the absolute value of .20 between effect sizes and the year of initial data collection, the length of follow-up, or the percentage of female participants in each study. However, the number of covariates included in multivariate models was moderately associated with effect size (r = ?.27). Visual inspection of the corresponding scatter plot indicated that when studies included seven or more covariates, effect sizes tended to be more homogeneous, without extremely high values. To clarify, the inclusion of many covariates did not substantively reduce the magnitude of the general findings, which tended to remain in the range of OR = 1.20?1.40, but it did eliminate all OR values greater than 1.66. Analyses also indicated that the association between the effect size and the average age of participants at intake was of a moderately strong magnitude (r = ?.34 for adjusted data, and r = ?.46 for unadjusted data). This association with participant age remained of the same magnitude when accounting for length of study followup (and participants’ age at the end of the study) and when age was or was not used as a statistical covariate. Examination of the scatter plot and breaking down the data into three approximately equal categories of initial participant age helped to interpret the correlation: Studies involving participants of an average age less than 65 years had an average effect size of OR = 1.57 for adjusted data, and OR = 1.92 for unadjusted data; studies involving participants of an average age between 65 and 75 years had an average effect size of OR = 1.25 for adjusted data, and OR = 1.32 for unadjusted data; and studies involving participants of an average age greater than 75 years had an average effect size of OR = 1.14 for adjusted data, and OR = 1.28 for unadjusted data. Adults less than 65 years of age appeared to be at greater risk of mortality when they lived alone or were lonely compared with older individuals in those same conditions, even after controlling for the effect of age and other covariates on mortality
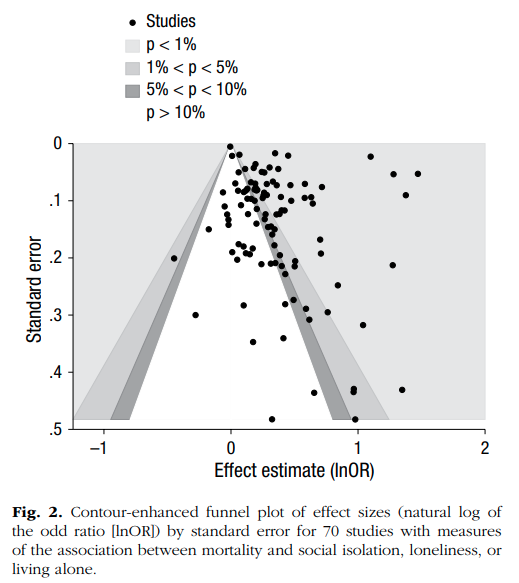
Fig. 2. Contour-enhanced funnel plot of effect sizes (natural log of the odd ratio [lnOR]) by standard error for 70 studies with measures of the association between mortality and social isolation, loneliness, or living alone.
Likelihood of publication bias adversely influencing the results
Publication bias occurs when the data obtained in a meta-analysis fail to represent the entire population of studies because of the increased probability of nonsignificant results remaining unpublished (and therefore less accessible for meta-analytic reviews). As can be seen in Figure 2, the data in this meta-analysis were highly variable, and the distribution of effect sizes appeared somewhat imbalanced toward the right side of the graph. The distribution of the data was relatively sparse toward the bottom of the white-shaded center of the graph, the area of nonsignificance. This kind of distribution can suggest that some nonsignificant studies were missing from the meta-analysis. However, neither Egger’s regression test nor an alternative to that test recommended for OR data (Peters, Sutton, Jones, Abrams, & Rushton, 2006) reached statistical significance (p > .05), which diminished the likelihood of possible publication bias. We found the fail-safe N?the number of hypothetically missing studies needed to reduce the present results to zero? to be 1,268, a number higher than the plausible number of studies conducted. Furthermore, using the trim and fill method (Duval & Tweedie, 2000), we did not estimate any “missing” studies; the distribution was overall fairly symmetric relative to the average effect size. It thus seemed unlikely that publication bias substantively affected the results of this meta-analysis.
Social isolation results in higher likelihood of mortality, whether measured objectively or subjectively. Cumulative data from 70 independent prospective studies, with 3,407,134 participants followed for an average of 7 years, revealed a significant effect of social isolation, loneliness, and living alone on odds of mortality. After accounting for multiple covariates, the increased likelihood of death was 26% for reported loneliness, 29% for social isolation, and 32% for living alone. These data indicated essentially no difference between objective and subjective measures of social isolation when predicting mortality. The prospective designs of these studies and the statistical models that controlled for initial health status (and several other potential confounds) provide evidence for the directionality of the effect. Although we cannot confirm causality, the data show that individuals who were socially isolated, lonely, or living alone at study initiation were more likely to be deceased at the follow-up, regardless of participants’ age or socioeconomic status, length of the follow-up, and type of covariates accounted for in the adjusted models. We caution scholars perusing the expanding research literature on the association of social isolation and loneliness with physical health against reliance on unadjusted data because those data fail to account for participant health status, a factor contributing to reverse causality (when individuals with impaired health report increased loneliness or social isolation because their health condition limits their social contacts). Averaged results with unadjusted data were of greater magnitude than the results from fully adjusted models (see Table 3), particularly when participants had a preexisting health condition and when physically ill participants were not excluded from the unadjusted analyses. In fully adjusted models accounting for health status and in studies with physically ill individuals removed from analyses (thus accounting for reverse causality), social isolation and loneliness remained predictive of mortality. Future researchers will need to confirm the hypothesis that when individuals are ill (and ostensibly needing support) their risk for mortality increases substantially when lacking social support.
Overall, the findings from this meta-analysis are consistent with prior evidence that has demonstrated higher survival rates for those who are more socially connected (Holt-Lunstad et al., 2010) and extend those findings by focusing specifically on measurement approaches that assess the relative absence of social connections. Notably, the present meta-analysis included more than double the number of studies and 10 times the number of participants compared with the previous meta-analysis. Thus, the field now has much stronger evidence that lacking social connections is detrimental to physical health. The average effect sizes identified in this meta-analysis were lower than those reported previously for measures of social networks (OR = 1.45, 95% CI [1.32, 1.59]) and social integration (OR = 1.52, 95% CI [1.36, 1.69]) and were much lower than complex measures of social integration (OR = 1.91, 95% CI [1.63, 2.23]; see Table 4 of Holt-Lunstad et al., 2010). This difference may suggest that the salubrious effects of being socially connected may be stronger than the adverse effects of lacking connections. However, it is also likely that research methods that account for the multidimensionality of social relationships better predict mortality than measurement focused on any single aspect of sociality, such as social isolation. Nonetheless, identification of the relative effects of each component may be useful in targeting those that may be modifiable. There is also presently no research evidence to suggest a threshold effect. The aggregate results suggest more of a continuum than a threshold at which risk becomes pronounced. Although it is possible that individuals who are extremely lonely or socially isolated may account for much of the elevated risk, presently too few researchers target extremely isolated individuals in studies. Given the complexity (including objective and subjective aspects) of social relationships, identifying such a threshold seems unlikely.
------
全体として、このメタアナリシスから得られた知見は、社会的つながりが強い人ほど生存率が高いことを示した先行証拠と一致し(Holt-Lunstad et al.、2010)、社会的つながりの相対的欠如を評価する測定アプローチに特に焦点を当てることでこれらの知見を拡張している。注目すべきは、今回のメタアナリシスでは、前回のメタアナリシスと比較して、研究数が2倍以上、被験者数が10倍以上となっていることである。したがって、この分野では、社会的つながりの欠如が身体的健康に有害であることを示す、より強力な証拠が得られたのである。 このメタ分析で確認された平均効果量は、社会的ネットワーク(OR = 1.45, 95% CI [1.32, 1.59] )と社会的統合(OR = 1.52, 95% CI [1.36, 1.69] )については前回報告したものより低く、社会統合の複合指標よりはるかに低かった(OR = 1.91, 95% CI [1.63, 2.23]; Holt-Lunstad et al.の表4参照, 2010)。この違いは、社会的なつながりがあることの有益な効果は、つながりがないことの有害な効果よりも強いことを示唆しているのかもしれない。しかし、社会的関係の多次元性を考慮した調査方法の方が、社会的孤立のような社会性の単一側面に焦点を当てた測定よりも死亡率をより良く予測できる可能性もある。それでも、各要素の相対的な効果を明らかにすることは、修正可能な要素に的を絞る上で有用であろう。また、現在のところ、閾値効果を示唆する研究証拠もない。集計結果は、リスクが顕著になる閾値というより、連続性を示唆している。極端に孤独な人、社会的に孤立した人がリスクの上昇の多くを占める可能性はあるが、現在のところ、極端に孤立した人を研究対象としている研究者が少なすぎる。社会的関係の複雑さ(客観的、主観的側面を含む)を考慮すると、そのような閾値を特定することは不可能と思われる。
------
Objective versus subjective isolation
Using the meta-analytic data, had we found that either social isolation or loneliness was more predictive of mortality, interventions to reduce risk could have become more targeted. However, we presently have no evidence to suggest that one involves more risk than the other for mortality. Unfortunately, in the vast majority of studies, researchers examined only one measurement approach (social isolation, loneliness, or living alone), precluding direct comparisons. Among the few studies in which researchers contrasted social isolation and loneliness, the evidence was mixed, with researchers finding that loneliness was more influential in one study (Holwerda et al., 2012), and with other researchers finding that social isolation had stronger effects than loneliness in a later study (Steptoe, Shankar, Demakakos, & Wardle, 2013). This inconsistency may be due to differences in methodological approaches to handling correlated psychological states, such as depression (Booth, 2000). Our analyses indicated that the elevated risk of mortality persisted even when controlling for correlated components of social networks and multiple other factors, including depression, with the use of covariates negating large effect sizes. In any case, the multiple, overlapping components of sociality make reliance on statistical adjustment less desirable than direct comparisons between components, such as loneliness and social isolation. The equivalent effects of social isolation and loneliness reported here do not indicate interchangeability of these risk assessments. Rather, the available data suggest that efforts to mitigate risk should consider both social isolation and loneliness without the exclusion of the other. Because social isolation and loneliness are often weakly correlated (Coyle & Dugan, 2012), simply increasing social contact may not mitigate loneliness. Likewise, exclusively altering one’s subjective perceptions among those who remain objectively socially isolated may not mitigate risk.
The evolutionary perspective of loneliness proposed by Cacioppo and colleagues (Cacioppo et al., 2006; Cacioppo, Cacioppo, & Boomsma, 2014) presents loneliness as an adaptive signal, similar to hunger and thirst, that motivates one to alter behavior in a way that will increase survival. Accordingly, loneliness is a powerful motivator to reconnect socially, which, in turn, increases survival and opportunity to pass on genes. Consistent with this perspective, intervention attempts to alter the signal (e.g., hunger, loneliness) without regard to the actual behavior (e.g., eating, social connection) and vice versa would likely be ineffective. Extending this possibility, some data have shown that those who are both high in loneliness and social isolation had the poorest immune response (Pressman et al., 2005). Therefore, both objective and subjective measures of social isolation should be considered in risk assessment. It is only through direct comparisons of social isolation and loneliness in the same sample that researchers can establish independent, relative, and synergistic effects. Consequently, it is possible that different combinations of social isolation and loneliness may represent different levels of risk. For instance, those low in both isolation and loneliness would presumably be at lowest risk, those high in both at highest risk, and those who are isolated but not lonely or lonely but not isolated to be at intermediate risk. Nonetheless, there is currently insufficient empirical evidence to test this hypothesis, highlighting an important weakness of the current literature that needs to be addressed in future research.
Cacioppoらが提唱する孤独の進化的視点(Cacioppo et al., 2006; Cacioppo, Cacioppo, & Boomsma, 2014)は、孤独を飢えや渇きと同様の適応的信号として示し、生存率を高めるように行動を変化させる動機付けとなるとしています。したがって、孤独は社会的なつながりを取り戻すための強力な動機づけとなり、その結果、生存率と遺伝子継承の機会が増加する。このような観点から、実際の行動(例:食事、社会的つながり)を無視してシグナル(例:空腹感、孤独感)を変える介入の試みは、おそらく効果がないだろう。この可能性を拡大すると、孤独感と社会的孤立感の両方が高い人は、免疫反応が最も悪いというデータもあります(Pressman et al.) 従って、リスク評価においては、社会的孤立の客観的、主観的な尺度の両方を考慮する必要があります。同じサンプルで社会的孤立と孤独を直接比較することによってのみ、研究者は独立した、相対的な、そして相乗的な効果を確立することができるのです。その結果、社会的孤立と孤独の異なる組み合わせが、異なるレベルのリスクを表している可能性があるのです。例えば、孤立と孤独の両方が低い人は最もリスクが低く、両方が高い人は最もリスクが高く、孤立しているが孤独ではない人、孤独だが孤立していない人は中間のリスクであると推測される。しかし、この仮説を検証する実証的証拠はまだ十分ではなく、現在の文献の重要な弱点が浮き彫りになっており、今後の研究で対処する必要がある。
------
Isolation and aging
The data in this meta-analysis should make researchers call into question the assumption that social isolation among older adults places them at greater risk compared with social isolation among younger adults. Using the aggregate data, we found the opposite to be the case. Middle-age adults were at greater risk of mortality when lonely or living alone than when older adults experienced those same circumstances. The moderating effect of age may seem counterintuitive in light of data indicating that individuals more than 65 years of age are more likely to report loneliness (Dykstra, van Tilburg, & de Jong Gierveld, 2005), but there are at least four plausible explanations for why middle-age adults may differ from older adults in terms of the relevance of social networks to physical health. First, it is possible that individuals who do not die early may be a particularly resilient group, with different social or health characteristics than those who die at earlier ages. Thus, the observed difference across age could be confounded with preexisting health status, although this interpretation is qualified by the fact that the researchers using multivariate statistical models accounted for participant age and health status. A second explanation involves changes in social networks as individuals transition from full-time employment to retirement, with decreases in socialization in occupational and public forums that are seen as culturally normative. This possible explanation is supported by one study in which researchers examined loneliness after retirement and found an effect for mental health (anxiety and depression) but not for physical health (functional status and number of chronic conditions; Bekhet & Zauszniewski, 2012). Third, it is plausible that individuals who are alone or lonely before retirement age may be more likely to engage in risky health behaviors or less likely to seek medical treatment early, whereas after retirement, people may attend more assiduously to their physical health.
------
孤立と老化
このメタ分析のデータは、高齢者の社会的孤立は若年者の社会的孤立よりもリスクが高いという仮定に疑問を投げかけるものである。集計データを用いて、我々はその逆であることを発見した。中年の成人は、高齢者が同じ状況を経験したときよりも、孤独または一人暮らしのときに死亡リスクが高くなることがわかった。 65歳以上の人は孤独を感じやすいというデータ(Dykstra, van Tilburg, & de Jong Gierveld, 2005)からすると、年齢の緩和効果は直感に反するように思われるが、身体の健康と社会ネットワークの関連性について、なぜ中年の成人が高齢者と異なるのかについては、少なくとも4つのもっともらしい説明がある。第一に、早期死亡しない人は、早期死亡する人とは異なる社会的特性や健康的特性を持つ、特に回復力の高い集団である可能性がある。したがって、年齢による違いは既存の健康状態と混同される可能性があるが、この解釈は、研究者が多変量統計モデルを用いて参加者の年齢と健康状態を説明したことによって限定されている。第二の説明は、常勤職から退職への移行に伴う社会的ネットワークの変化と、文化的に規範的とみなされる職業上および公的な場での社会化の減少が関係しているというものである。この説明は、退職後の孤独感を調査したある研究で支持されており、精神的健康(不安と抑うつ)には影響があったが、身体的健康(機能的状態や慢性疾患の数)には影響がなかったという。第三に、定年前に孤独であった人は、リスクの高い健康行動をとりやすい、あるいは早期に治療を受けにくいという可能性があり、一方、定年後は身体の健康により熱心に取り組むという可能性がある。
------
Finally, it is possible that the different results across participant age are confounded with marital status: Older adults are much more likely to be widows/widowers than middle-age adults. Our metaanalysis cannot shed light on these four possible explanations because the first three explanations involve variables inadequately evaluated in the present research literature, and the variable associated with the fourth explanation, marital status, was not coded in our analyses. Although many studies indicate that loneliness differs across marital status (Cacioppo & Patrick, 2008; Hughes et al., 2004; Victor & Bowling, 2012) and that marital status is significantly associated with mortality (Roelfs, Shor, Kalish, & Yogev, 2011), we did not include marital status as an indicator of social isolation because being unmarried does not necessarily mean that one is socially isolated, living alone, or lonely. Moreover, there would be multiple qualitative differences in the social networks of an older individual who had never been married compared with one who had been married and raised children but whose spouse had recently died, even though both are living alone. Rather than include all possibly correlated variables (e.g., marital status, depression, substance abuse), we evaluated only direct measures of social isolation, living alone, or loneliness. Given the limitations of the present meta-analysis, future researchers should confirm the apparent differences across participant age and should evaluate the relative merits of the several plausible explanations for that finding
To better evaluate differences across age, future researchers should involve participants from a broad range of age groups. Most of the data in this meta-analysis came from older adults. Only 24% of studies involved people with an average age of 59 years or younger, and only 9% of studies involved people younger than 50 years of age at intake. If future data collection with younger adult samples confirms the age differences we observed in this meta-analysis, then widespread beliefs about the health risks of social isolation being greatest among older adults are inaccurate. In any case, the metaanalytic data, taken together with evidence for detrimental influences across the life span (Qualter et al., 2015, this issue), suggest that future research (and possibly interventions) should expand beyond older adults.
Substantial evidence now indicates that individuals lacking social connections (both objective and subjective social isolation) are at risk for premature mortality. The risk associated with social isolation and loneliness is comparable with well-established risk factors for mortality, including those identified by the U.S. Department of Health and Human Services (physical activity, obesity, substance abuse, responsible sexual behavior, mental health, injury and violence, environmental quality, immunization, and access to health care; see www.hhs.gov/safety/index). A substantial body of research has also elucidated the psychological, behavioral, and biological pathways by which social isolation and loneliness lead to poorer health and decreased longevity (for reviews, see Cacioppo, Cacioppo, Capitanio, & Cole, 2015, this issue; Shankar et al., 2011; Thoits, 2011; see also Cacioppo et al., 2015; Hawkley & Cacioppo, 2003, 2010). In light of mounting evidence that social isolation and loneliness are increasing in society (McPherson & Smith-Lovin, 2006; Perissinotto, Stijacic Cenzer, & Covinsky, 2012; Victor & Yang, 2012; Wilson & Moulton, 2010), it seems prudent to add social isolation and loneliness to lists of public health concerns. The professional literature and public health initiatives can accord social isolation and loneliness greater recognition.
------
結論
社会的なつながりのない人(客観的、主観的な社会的孤立)は早期死亡のリスクがあることを示す証拠は十分にある。社会的孤立や孤独に関連するリスクは、米国保健社会福祉省が特定したものを含む、確立された死亡の危険因子(身体活動、肥満、物質乱用、責任ある性行動、精神衛生、怪我と暴力、環境の質、予防接種、医療へのアクセス; www.hhs.gov/safety/index を参照)と同等である。また、多くの研究が、社会的孤立と孤独がより悪い健康と長寿の減少につながる心理的、行動的、生物学的経路を解明してきました(レビューとして、Cacioppo, Cacioppo, Capitanio, & Cole, 2015, this issue; Shankar et al.) 社会的孤立と孤独が社会で増加しているという証拠の積み重ねを考慮すると(McPherson & Smith-Lovin, 2006; Perissinotto, Stijacic Cenzer, & Covinsky, 2012; Victor & Yang, 2012; Wilson & Moulton, 2010)、公衆衛生に関するリストの中に社会的孤立と孤独を追加することは賢明であるように思われます。専門的な文献や公衆衛生の取り組みは、社会的孤立や孤独をより認識させることができます。
------
To draw a parallel, several decades ago scientists who observed widespread dietary and behavior changes (increasing consumption of processed and calorie-rich foods and increasingly sedentary lifestyles) raised warnings about obesity and related health problems (e.g., Brewster & Jacobson, 1978; Dietz & Gortmaker, 1985). The present obesity epidemic (Wang & Beydoun, 2007) had been predicted. Obesity now receives constant coverage in the media and in public health policy and initiatives. The current status of research on the risks of loneliness and social isolation is similar to that of research on obesity 3 decades ago?although further research on causal pathways is needed, researchers now know both the level of risk and the social trends suggestive of even greater risk in the future. Current evidence indicates that heightened risk for mortality from a lack of social relationships is greater than that from obesity (Flegal, Kit, Orpana, & Graubard, 2013; Holt-Lunstad et al., 2010), with the risk from social isolation and loneliness (controlling for multiple other factors) being equivalent to the risk associated with Grades 2 and 3 obesity. Affluent nations have the highest rates of individuals living alone since census data collection began and also likely have the highest rates in human history, with those rates projected to increase (e.g., Euromonitor International, 2014). In a recent report, researchers have predicted that loneliness will reach epidemic proportions by 2030 unless action is taken (Linehan et al., 2014). Although living alone can offer conveniences and advantages for an individual (Klinenberg, 2012), this meta-analysis indicates that physical health is not among them, particularly for adults younger than 65 years of age. Further research is needed to address the complexities of social interactions, interdependence, and isolation (Parigi & Henson, 2014; Perissinotto & Covinsky, 2014), but current evidence certainly justifies raising a warning.